Vivek Y. Reddy, MD; Steven Castellano, PhD; Petr Neuzil MD, PhD; Atul Verma, MD; Melissa H. Kong, MD
Background
Since the STAR-AF II trial, there has been a trend toward PVI-only ablation strategies for persistent AF (PeAF). Electrographic Flow (EGF) mapping can identify active sources of AF and can also estimate the consistency of wavefront propagation through the atrium. Electrographic flow consistency (EGFC) is the Euclidean length of a sequence of vector field estimates of observed wavefront activation patterns and combined with EGF-identified sources may aid in optimizing ablation strategies based on functional AF
mechanisms for PeAF as ablation limited to pulmonary vein isolation (PVI) would not be expected to adequately treat all patients.
Objectives
Examine the success of a PVI-only ablation strategy for a redo PeAF/long-standing PeAF population.
Methods
FLOW-AF (NCT04473963) prospectively enrolled non-paroxysmal AF patients undergoing redo ablation at 4 centers. One minute EGF recordings using a 64-pole basket catheter were obtained both pre-PVI and post-PVI after a 20-minute wait and confirmation of electrical isolation. Patients with EGF-identified source activity (SAC) ≥26.5% were randomized 1:1 to EGF-guided source ablation v. PVI-only; if SAC<26.5% patients mostly received PVI-only.
Results
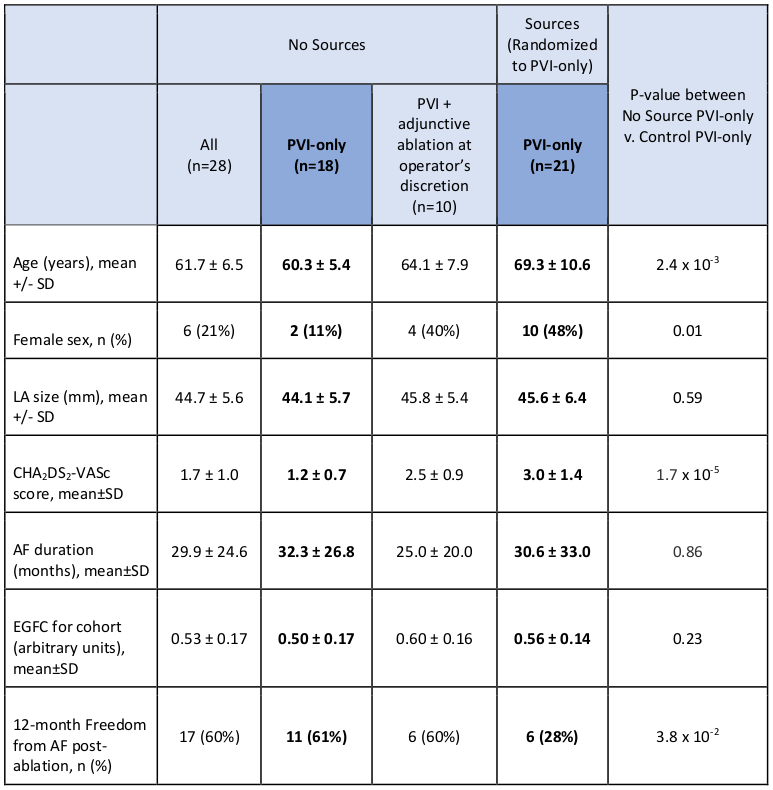
Prospective study of 85 patients enrolled: 23 with sources randomized to PVI-only (Sources Randomized to Control) and 32 not randomized who were assigned to PVI-only (No Sources). Of the 32 non-randomized patients, 21 received strictly PVI-only and 11 underwent PVI plus adjunctive ablation such as posterior wall isolation or left atrial roof line at the operator’s discretion. Baseline demographics in Table. Of all patients who received strictly PVI-only, those with No Sources v. Sources had significantly different clinical characteristics including older age, more women, and higher CHA2DS2-VASc in the Sources group. Mean EGFC between patients with No Sources v. Sources was not significantly different (0.50±0.17 v. 0.56±0.14, p=0.23). However, after PVI-only, those with No Sources had 61% FFAF (11/18) v. those with unabated Sources who had 28% (6/21) FFAF, p=3.8×10-2.
Conclusions
Success rate in No Sources group with PVI-only is better than success rate in those with Sources randomized to PVI-only. For the clinically heterogenous population of PeAF patients, PVI-only will not be enough for all patients.