Patricia Chen; Boaz Avitall, MD, PhD; Josef Koblish; Julie Mou; Ken Berliner; Donghoon Chun, Ph.D; Ken S. Lizama, MD, Melissa H. Kong, MD
Background
Pulse field ablation (PFA) is a promising energy modality for cardiac ablation due to its speed, tissue selectivity, and potential ability to create consistent transmural lesions.
Objective
Evaluate PFA lesions created using an innovative catheter design combining focal, linear and pulmonary vein (PV) ablation.
Methods
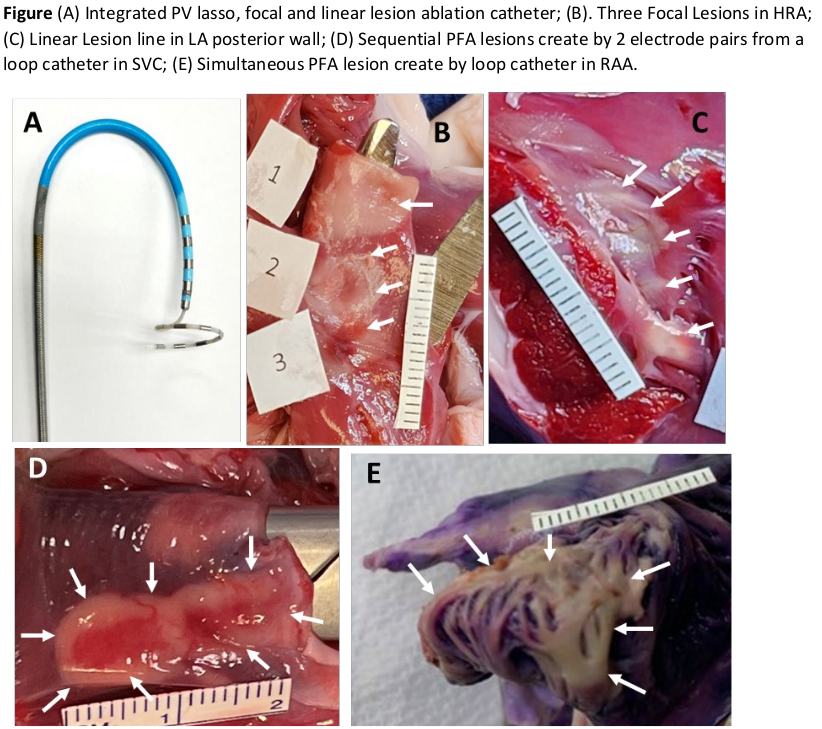
PEF ablation was performed using an 8F bidirectional linear catheter with a 2mm tip and 4 ring electrodes through which a 3.5F loop catheter (6 to 9 rings, 3mm length on 19mm diameter) can be inserted and deployed beyond the tip (Figure, A).
In 8 swine, R-wave gated biphasic pulse trains of voltage between 600 and 700V were delivered sequentially and simultaneously to the loop or linear catheter electrode pairs. The linear catheter is compatible with any commercially available 8.5F transseptal sheath. Porcine intracardiac tissue was ablated in vivo targeting the superior vena cava (SVC), right atrium (RA), RA appendage (RAA), cavotricuspid isthmus, left atrium, PVs, and right ventricle. Electrogram (EGM) amplitudes/morphology and pre- and post-ablation pacing thresholds were assessed. Triphenyl tetrazolium chloride (infused 20 minutes before euthanasia) or tetrazolium blue stain was used to demarcate and measure the lesions
Histopathologic analysis of all cardiac tissues was performed, esophageal pre and post ablation phrenic nerve stimulation were done.
Results
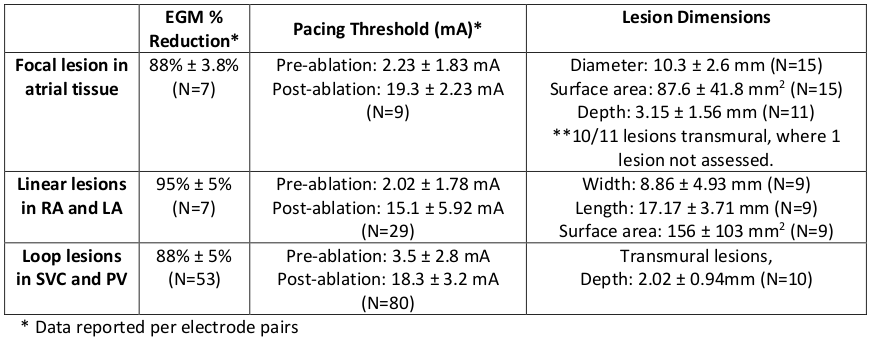
EGM attenuation and pacing thresholds increased were documented (see Table).
Focal: PFA was delivered from the distal electrode pair of the linear catheter. Lesion measured 10.3 ± 2.6 mm diameter, 3.15 ± 1.56 mm depth (Figure, B).
Linear: PFA was delivered to 5 electrodes of the linear catheter (Figure, C). Lesion dimension range: width: 4-20mm, length: 12 to 20mm
Loop: PFA was delivered sequentially via loop catheter electrode pairs to PVs resulting in transmural lesions with 2.02 ± 0.94mm depth measured at the thickest area of affected myocardium (Figure, D).
Simultaneous biphasic PEF was delivered by loop electrode pairs to the RAA and SVC, resulting in transmural lesions. RAA lesion measured 132mm2 surface area with average EGM attenuation 87% ± 2% and pacing thresholds increased post ablation(p=0.00), 4.0±2.1 mA pre, 18.5±4.2 mA post (Figure, E). No esophageal or phrenic injuries were documented.
Conclusion
The combined linear, focal, and circular PFA ablation device demonstrated acute lesion success and each configuration has the potential to create effective transmural lesions in the atrium.