Sandeep Goyal, MD; Steven Castellano, PhD; Melissa Kong, MD; Kent Nilsson, MD, PhD; Pawel Derejko, MD; Tamas Szili-Torok, MD, PhD; Atul Verma, MD; Mohit Turagam, MD
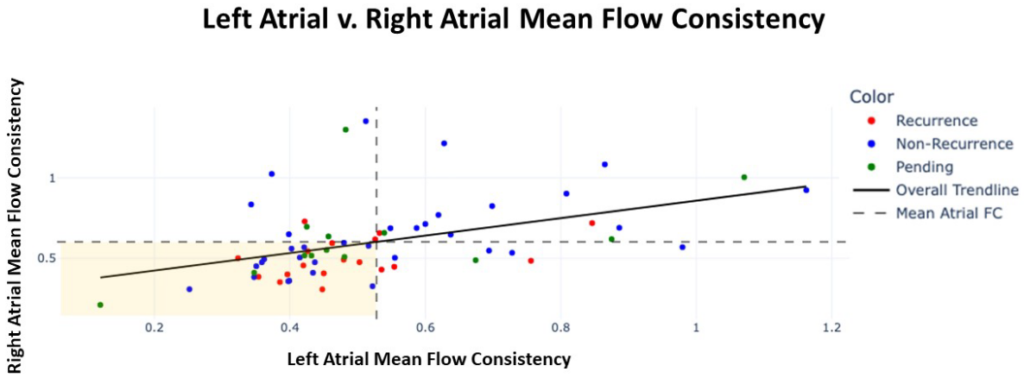
FC. The vertical dashed line indicates the LA mean FC and the horizontal dashed line is the RA mean FC.
The majority of patients with recurrent AF within 1 year post-ablation (red dots) have FC below the
mean in both the LA and the RA (lower left quadrant). Green dots represent patients for whom
outcome is not yet available and those falling in the lower left quadrant would be predicted to be more
likely to have AF recurrence within 1 year post-ablation than those falling in any other quadrant.
Background
Arrhythmogenic atrial structural remodeling tends to start near the ostia of the pulmonary veins (PVs) and then progress to other regions of the left atrium (LA) before affecting the right atrium (RA) in patients with atrial fibrillation (AF). Electrographic Flow (EGF) mapping visualizes global cardiac wavefront propagation in near real-time. The nature of atrial substrate may be assessed with flow vectors using electrographic flow consistency (FC), which is the magnitude of vector flow at all points in space and time. High FC characterizes stable wavefront propagation through a particular region of the endocardium while low FC indicates more chaotic and disorganized wavefront propagation.
Objectives
Examine patterns of FC between the LA and RA among all-comers with AF.
Methods Data was prospectively collected from patients with paroxysmal, persistent, and long-standing persistent AF, who underwent EGF mapping with a 64-electrode basket catheter and catheter ablation for AF. For each patient, a series of 1 minute EGF recordings were taken post-PVI in multiple standardized locations in both LA and RA to optimize endocardial coverage. Recordings always occurred prior to any EGF-identified source ablations, if clinically relevant sources were detected post-PVI. Mean FC from these recordings were taken and averaged per recording location and then averaged per
atrium.
Results
Prospective study of 65 patients enrolled: mean age 63.0 ± 9.4 years, 28% (18/65) female, mean LAD 44.4 ± 5.6 mm. Mean FC was higher in RA v. LA (0.60±0.23 v. 0.53±0.19, p=0.026). A linear relationship was established between RA and LA FC means (m=0.51, r=0.42, p=2.0×10-4), suggesting that as FC decreases in LA, FC decreases only half (51%) as much in RA. Slope and r were unaffected by recurrence status of patients. Of the 65 patients, 12-month post-ablation outcomes were available for 52: recurrence rate was 61% (11/18) in patients with FC below the mean in both LA and RA v. 11% (2/18) in patients with FC above the mean in both atria.
Conclusions
With progressive substrate remodeling, mean electrographic FC decreases and mean FC is lower in LA than RA, which may reflect that pathophysiologically, fibrosis tends to originate in LA and spread to RA. FC below the mean in both atria may indicate biatrial disease with more progressive substrate remodeling and hence worse outcomes. More outcomes data is required to understand the utility of biatrial FC as a marker for AF disease.